















 611 692
611 692

was underpowered, it nonetheless suggests that selection
bias in retrospective analyses may be driving findings
suggesting superiority for PN in terms of oncologic survival
outcomes. A similar study for larger masses is still lacking,
and has recently been advocated
[8]. While we support the
concept of a prospective randomized trial comparing RN
and PN for oncologic efficacy in larger renal masses in which
predetermined eligibility criteria can limit potential selec-
tion bias, it is nonetheless instructive and illuminating to
evaluate the evidence currently available from several large
comparative retrospective analyses, even if the ultimate
conclusions that may be drawn with respect to superiority
require tempering in light of the findings from EORTC
30904.
Our pooled analysis confirms that RN cases are
substantially higher in number than PN in this specific
clinical setting (RN 8620; PN 2584), confirming trends
reported by others
[11,12]. In our analysis, patients
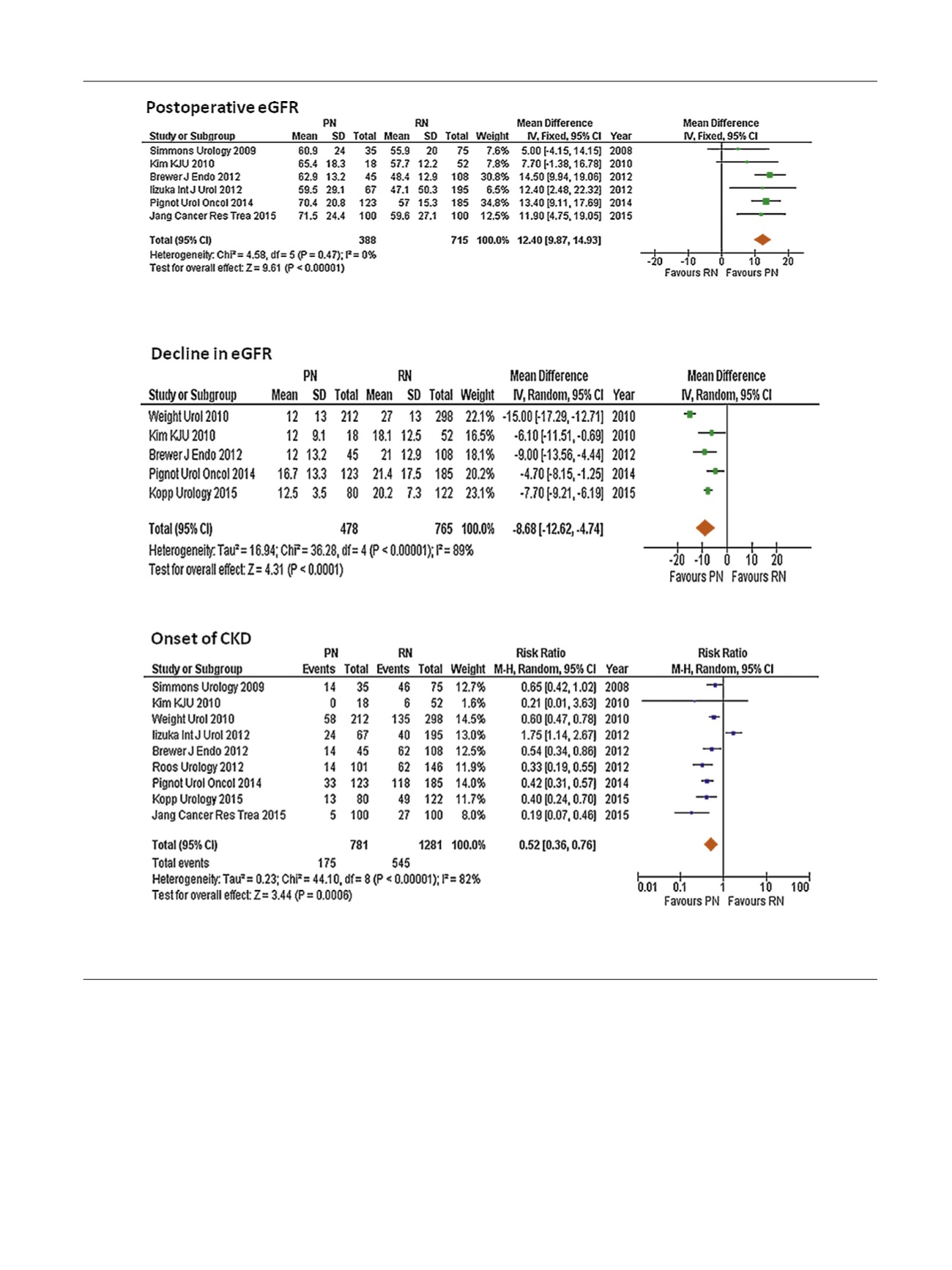
[(Fig._3)TD$FIG]
Fig. 3 – Forest plots of functional outcomes for partial nephrectomy (PN) versus radical nephrectomy (RN) for cT1b and cT2 tumors. Reference numbers
for the studies are shown in
Table 1 .eGFR = estimated glomerular filtration rate; CKD = chronic kidney disease; SD = standard deviation; CI = confidence
interval.
E U R O P E A N U R O L O G Y 7 1 ( 2 0 1 7 ) 6 0 6 – 6 1 7
611