















 610 692
610 692

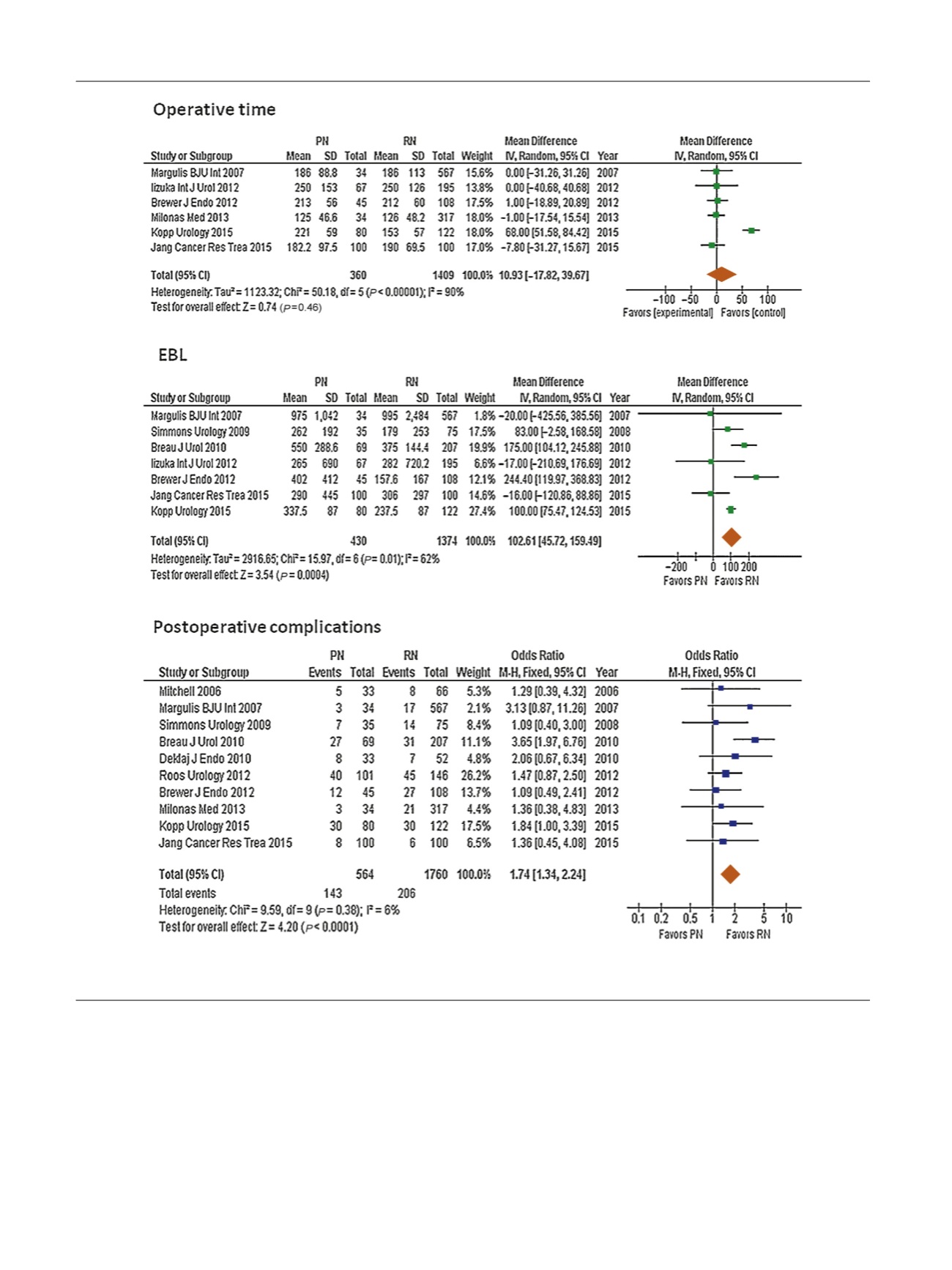
more technically demanding procedure, as demonstrated
by higher odds of complications. However, this higher
surgical risk is counterbalanced by the similar efficacy of PN
to RN in providing effective cancer control, with the notable
advantage of allowing better preservation of renal function.
Despite its shortcomings in terms of design and
implementation, EORTC 30904 remains the only prospec-
tive randomized trial comparing PN and RN for kidney
cancer to date. Its findings have generated significant
debate, as the expected superiority of PN over RN for overall
survival was not confirmed
[44] ,despite demonstration of
the expected benefits in terms of renal function preserva-
tion
[6]. Indeed, the findings of EORTC 30904, while limited
to masses of
<
5 cm, need to be placed in context, and first
and foremost demonstrate oncologic equivalence between
RN and PN for renal cell carcinoma. Second, while the study
[(Fig._2)TD$FIG]
Fig. 2 – Forest plots of surgical outcomes for partial nephrectomy (PN) versus radical nephrectomy (RN) for cT1b and cT2 tumors. Reference numbers
for the studies are shown in
Table 1 .EBL = estimated blood loss; SD = standard deviation; CI = confidence interval.
E U R O P E A N U R O L O G Y 7 1 ( 2 0 1 7 ) 6 0 6 – 6 1 7
610