















 621 692
621 692

PSA is a continuous parameter, with higher levels indicating
greater likelihood of PCa, precluding an optimal PSA
threshold for detecting nonpalpable but clinically signifi-
cant PCa. A limited PSA elevation alone should be confirmed
after a few weeks under standardised conditions (ie, no
ejaculation, manipulations, and urinary tract infections) in
the same laboratory before considering a biopsy. The
empiric use of antibiotics in an asymptomatic patient
should not be undertaken
[22].
The free-to-total PSA ratio stratifies the risk of PCa in
men with 4–10 ng/ml total PSA and a previous negative
biopsy but may be affected by several preanalytical and
clinical factors (eg, instability of free PSA at 4
8
C and room
temperature, variable assay characteristics, and large
concomitant benign prostatic hyperplasia [BPH]). Novel
assays for risk stratification measuring a panel of kallikreins
including the Prostate Health Index test and the four-
kallikrein score test are intended to reduce the number of
unnecessary biopsies in men with a PSA between 2 and
10 ng/ml. Prospective multicentre studies demonstrated
that both tests outperformed free-to-total PSA for PCa
detection
[23,24]. A formal comparison of these new tests is
lacking.
5.
Prostate biopsy
TRUS-guided biopsy using an 18G biopsy needle and a
periprostatic block is the standard of care. When the same
number of cores are taken, both transrectal and transper-
ineal approaches have comparable detection rates
[25,26].
Ten- to 12-core biopsies should be taken, bilateral from
apex to base, as far posterior and lateral as possible from the
peripheral gland. Additional cores should be obtained from
DRE/TRUS suspect areas. Oral or intravenous quinolones are
state-of-the-art preventive antibiotics, in spite of the
increased resistance to quinolones, which is associated
with a rise in severe infectious complications
[27]. Other
biopsy complications include haematospermia (37%), hae-
maturia lasting
>
1 d (14.5%), and rectal bleeding lasting 2
d (2.2%). Each biopsy site should be reported individually,
including its location, the ISUP 2005 GS, and extent. ISUP
2014 grade should be given as a global grade, taking into
account the Gleason grades of cancer foci in all biopsy sites.
If identified, intraductal carcinoma, lymphovascular inva-
sion, perineural invasion, and extraprostatic extensionmust
each be reported.
Table 5summarises the indications for
repeat biopsy following an initial negative biopsy.
Many single-centre studies suggest that multiparametric
magnetic resonance imaging (mpMRI) can reliably detect
aggressive tumours with a negative predictive value (NPV)
and positive predictive value ranging from 63% to 98% and
from 34% to 68%, respectively
[28]. The combination of
systematic and targeted biopsies (MRI-Tbx) may also better
predict the final GS
[29]. As a result, some authors proposed
performing systematic mpMRI before a prostate biopsy
[30,31]. One meta-analysis suggested that MRI-Tbx had a
higher detection rate of clinically significant PCa compared
with TRUS biopsy (sensitivity 0.91 vs 0.76) and a lower rate
of detection of insignificant PCa (sensitivity 0.44 vs 0.83).
However, this benefit was restricted to the repeated biopsy
subgroup
[32]. Two more recent randomised controlled
trials (RCTs) restricted to the initial biopsy yielded
contradictory results regarding the added value of MRI-
Tbx combined with systematic biopsies
[33,34]. Major
limitations of mpMRI are its interobserver variability and
the heterogeneity in the definitions of positive and negative
examinations. The first version of the Prostate Imaging
Reporting and Data System (PI-RADS) scoring system failed
to improve interobserver variability as compared with
subjective scoring
[35]. An updated version (PI-RADS v2)
needs to be evaluated further
[36].
6.
Staging of prostate cancer
The decision to proceed with a further staging work-up is
guided by which treatment options are available, taking
into account the patient’s preference and comorbidity. A
summary of the guidelines is presented in
Table 6.
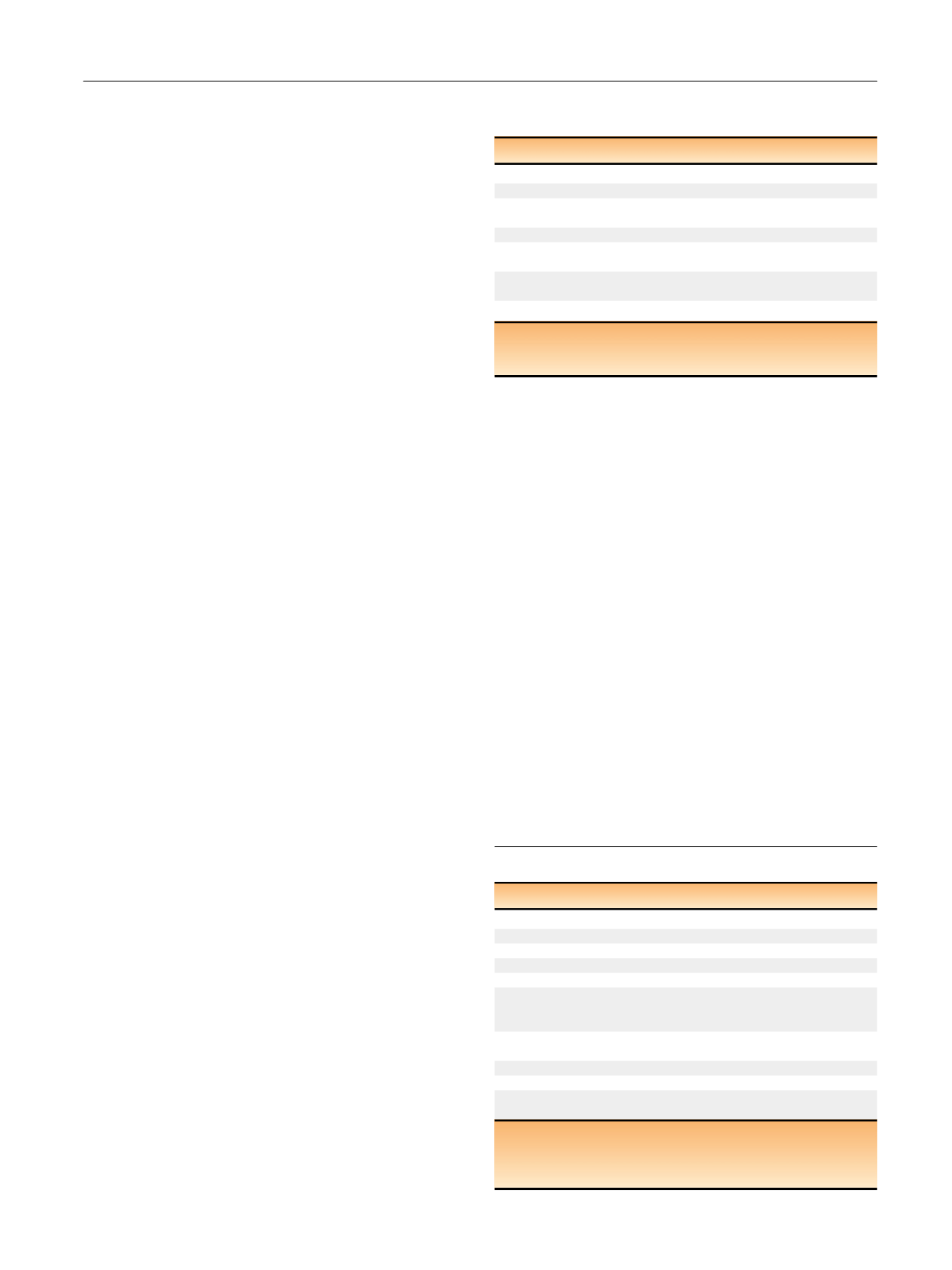
Table 6 – Guidelines for staging of prostate cancer
Risk group
LE GR
Any risk group staging
Do not use CT and TRUS for local staging
2a A
Low-risk localised PCa
Do not use additional imaging for staging purposes
2a A
Intermediate-risk PCa
In predominantly Gleason pattern 4, metastatic screening,
include at least cross-sectional abdominopelvic imaging
(s.a. CT/MRI) and a bone scan for staging purposes
2a A*
In predominantly Gleason pattern 4, use prostate mpMRI
for local staging
2b A
High-risk localised PCa or high-risk locally advanced PCa
Use prostate mpMRI for local staging
2b A
Perform metastatic screening including at least cross-sectional
abdominopelvic imaging and a bone-scan
2a A
CT = computed tomography; GR = grade of recommendation; LE = level of
evidence; mpMRI = multiparametric magnetic resonance imaging; MRI =
magnetic resonance imaging; PCa = prostate cancer; TRUS = transrectal
ultrasound.
Table 5 – Indications for rebiopsy after a negative biopsy and the
associated risk to find a prostate cancer
Indication
Associated PCa risk
Rising and/or persistently elevated PSA
–
Suspicious DRE
5–30%
Atypical small acinar proliferation
(ie, atypical glands suspicious for cancer)
40%
Extensive (ie, 3 biopsy sites) high-grade PIN
30%
Few atypical glands immediately adjacent to
high-grade PIN
50%
Intraductal carcinoma as a solitary finding
>
90% (mainly
high-grade PCa)
Positive mpMRI
34–68%
DRE = digital rectal examination; mpMRI = multiparametric magnetic
resonance imaging; PCa = prostate cancer; PIN = prostatic intraepithelial
neoplasia; PSA = prostate-specific antigen.
E U R O P E A N U R O L O G Y 7 1 ( 2 0 1 7 ) 6 1 8 – 6 2 9
621