















 644 692
644 692

1.
Introduction
Laparoendoscopic single-site (LESS) renal surgery, including
radical nephrectomy (RN) and partial nephrectomy (PN),
offers several advantages over the standard multiport
approach, namely improved cosmesis, less postoperative
pain, and faster recovery
[1]. Unfortunately, conventional
LESS is fraught with technical challenges, including in-line
vision, reverse handedness, loss of triangulation, and
instrument clashing, which have limited its dissemination
[2,3] .The application of the standard robotic platform to
LESS (R-LESS) addressed some but not all of these limitations
[4] .The largest contemporary study comparing R-LESS PN
to multiport robotic PN reported inferior trifecta outcomes
for R-LESS, demonstrating the limitations of a non–
purpose-built robotic platform for R-LESS
[5]. Two prior
generations of task-specific, single-site robotic platforms
have been developed to address these challenges. The
second-generation single-site robotic system successfully
overcame the instrument clashing and space constraints of
prior systems through the use of three articulating
endoscopic instruments and an articulating endoscopic
camera introduced via a single robotic port. Despite the
improvements offered by this system, maneuverability
within the working space was still restricted owing to the
fixed position of the robotic arms at their entrance to the
body
[6] .Standard robotic and R-LESS renal surgery is commonly
performed via a transperitoneal approach because of the
large working space and familiar landmarks of the
peritoneal cavity. A retroperitoneal approach has been
advocated for minimally invasive PN to avoid bowel
mobilization and expedite recovery; however, technical
constraints have hindered adoption and limited application
to polar or posterolateral tumors
[7,8].
We sought to evaluate the latest purpose-built single-
site robotic surgical platform, designed specifically for
extraperitoneal R-LESS surgery, in performing retroperito-
neal RN and PN in a cadaveric model.
2.
Materials and methods
2.1.
Objective and outcome measures
The primary objective of this experimental study was to determine the
feasibility of RN and PN using the new single-site robotic platform, as
measured by the rate of conversion to alternative approaches, operative
times, and occurrence of intraoperative complications. An intraoperative
complication was defined as any accidental puncture or laceration to an
organ, hollow viscus, or vessel. For PN, since the kidneys did not contain
tumors, the maximum diameter of the resected parenchyma was
measured and recorded as the excision size.
2.2.
Third-generation da Vinci SP surgical system
The new da Vinci SP surgical system (model SP1098; Intuitive Surgical,
Sunnyvale, CA, USA) represents an evolution of the second-generation
robotic system (SP999) with upgraded technology designed specifi-
cally for extraperitoneal single-site surgery
( Fig. 1 ) [6]. The improve-
ments include enhanced high-definition three-dimensional optics and
intelligent instrument arm control. Similar to the SP999, the SP1098
consists of three main components: a surgeon console, a patient side cart,
and a vision cart. The designs of the articulating endoscopic camera and
three double-jointed articulating endoscopic instruments, which enter
the patient through a multichannel robotic port, are unchanged. As before,
four robotic manipulators, or instrument drives, that control the camera
and instruments are mounted on an instrument arm that is attached to
the patient side cart
( Fig. 2). The surgeon console is identical to the
second-generation robotic system (SP999) with a foot pedal that allows
control of the instrument arm. Unique to this robotic system is the ability
to clutch and pivot the instrument arm about its remote center without
moving each individual instrument. In effect, an instrument can be
stationed at one location in the surgical field (eg, for retraction) while the
instrument arm is clutched and reoriented to a separate site, where the
remaining instruments can be deployed without disturbing the stationary
instrument. This improvement overcomes the constraint of multiple
instruments entering the body through a fixed point, effectively
expanding the workspace and improving maneuverability. The new
vision cart is similar to the previous generation with upgraded resolution
to accommodate the improved camera optics.
2.3.
Surgical technique
The cadavers were placed in a full (90
8
) flank position and secured to the
operating table. A 2.5-cm transverse skin incision was made 2 cm
anterior and inferior to the tip of the 12th rib, and dissection was carried
down through the subcutaneous tissues. The flank musculature was
identified and split, exposing the thoracolumbar fascia. The fascia was
incised and the retroperitoneum was entered. A novel 25-mm
multichannel robotic port was inserted into the retroperitoneal opening,
and the retroperitoneal space was developed. This proprietary port
accommodates an oval articulating camera (12 mm 10 mm), three 6-
mm double-jointed articulating instruments, and a 8-mm accessory port
for the introduction of sutures and suctioning. The robot was docked.
The surgical steps were performed according to our previously
described technique
( Fig. 3)
[9,10]. For PN, the retroperitoneal space was
fully developed; the hilumwas identified and prepared for clamping; the
kidney surface was exposed; the line of excision was marked with
cautery; the hilum was clamped; and renal excision and reconstruction
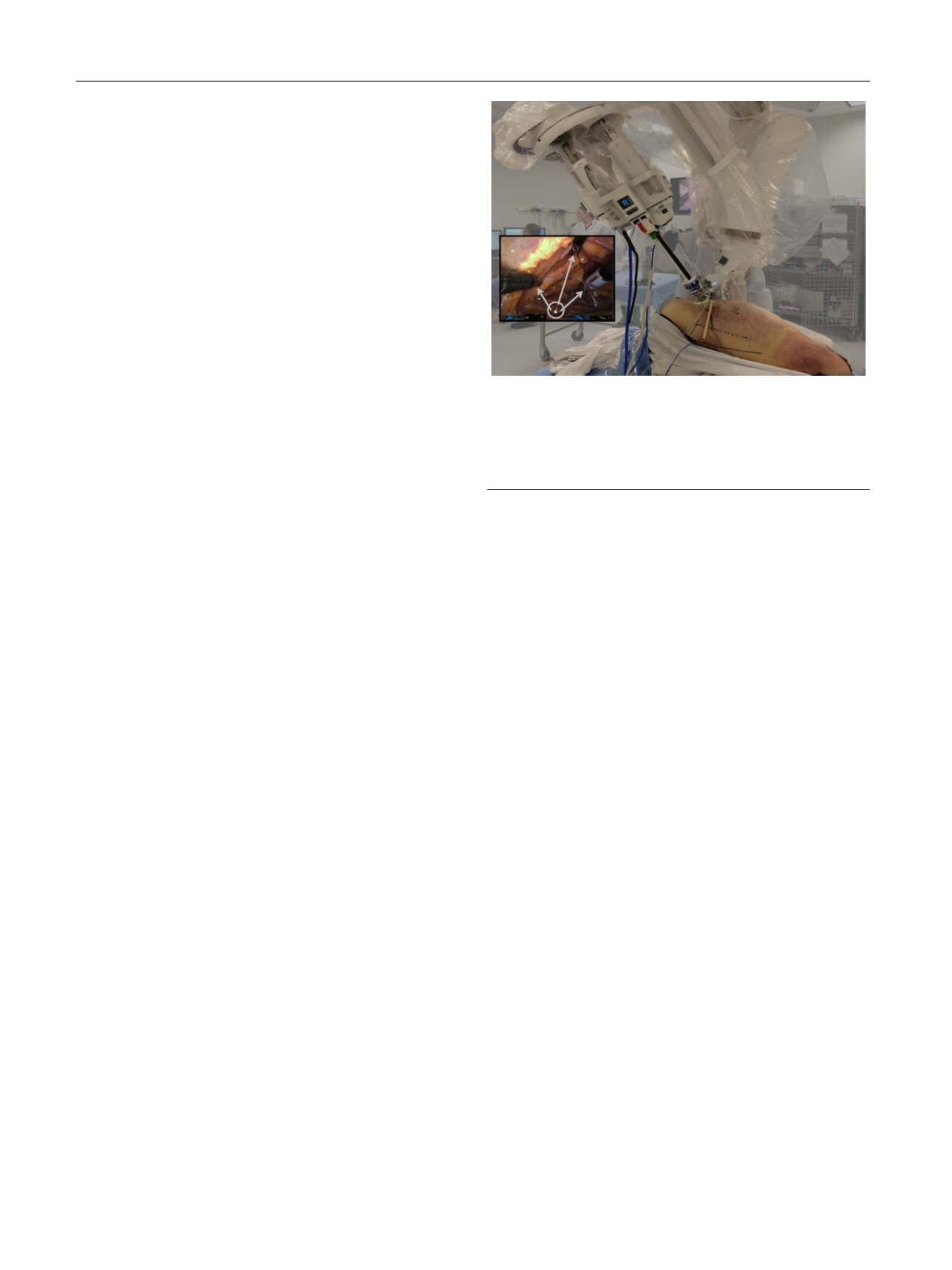
[(Fig._1)TD$FIG]
Fig. 1 – The da Vinci SP1098 surgical system (Intuitive Surgical,
Sunnyvale, CA, USA). The inset is an intraoperative view showing the
instrument compass (circle), which demonstrates the location of the
robotic instruments (arrows) within the surgical field. The instrument
icon turns orange when the instrument is near the limit of reach, and
red when the instrument has reached its limit.
E U R O P E A N U R O L O G Y 7 1 ( 2 0 1 7 ) 6 4 3 – 6 4 7
644